 Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY



 Indexed Articles
Indexed ArticlesSelect your language of interest to view the total content in your interested language
K. Karavdić1*, E. Milišić1, I. Abdagić2, A. Smajić2, A. Mešić2, D. Udovičić-Gagula3
1Clinic for Pediatric Surgery, Clinical Center of University Sarajevo, Patriotske lige 81, 71000 Sarajevo, Bosnia and Herzegovina
2Clinic for Anesthesia and renimation, Clinical Center of University Sarajevo, Bolnička 25, 71000 Sarajevo, Bosnia and Herzegovina
3Institute of Clinical Pathology, Clinical Center of University Sarajevo, Bolnička 25, 71000 Sarajevo, Bosnia and Herzegovina
Corresponding author: Karavdić K, Department of Pediatric Surgery, Clinical Center of University Sarajevo, Bosnia and Herzegovina, Bosnia;
E-mail: kenan.kv@bih.net.ba
Received date: December 29, 2019; Accepted date: January 07, 2020; Published date: January 17, 2020
Citation: Karavdić K, Milišić E, Abdagić I, et al. (2020) 360 Degree Twisted Transverse Colon in a Neurological Impaired Girl with a History of Chronic Constipation - A Case Report. J Med Res Surg 1(1): pp. 1-4.
Copyright: © 2020 Karavdić K. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which
permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Introduction: Transverse colon volvulus is an uncommon cause of bowel obstruction. Predisposing factors are mental retardation, dysmotility disorders, chronic constipation, and congenital megacolon.
Case report: We presented a transverse colon volvulus in a 14-year-old girl with mental retardation. Chronic constipation in neurologically impaired patients was a risk factor predisposing to volvulus. The girl was admitted to our Clinic because of problems that last 4-5 days and was followed by abdominal pain, vomiting and lack of stool. Vomiting was once a day. She was sub febrile up to 37.6°C. On examination, the abdomen was distended, tense, diffusely painful. During the surgery, a 360° clockwise volvulus of the transverse colon was found. After the reduction of volvulus, an enormous transverse colon was resected and protective ileostomy was formed. In the postoperative period, ileostoma functioned a good. The definitive surgical treatment was done on the 20th postoperative day when the occlusion of the ileostomy and transanal biopsy of the rectum was done, which showed the presence of ganglia cells. The patient was discharged from our institution after 1 month.
Conclusion: Pediatric patient with neurological conditions and mental retardation present an increased risk of colon transversum volvulus due to chronic obstruction.
Transverse colon volvulus, Mental retardation, Ileostomy
Transverse colonic volvulus in children is a rare condition with an unknown incidence [1-5]. Less than 30 cases of pediatric transverse volvulus have been reported in the literature. Bowel obstruction due to colonic volvulus in adults represents 3-5% of all cases [1]. The most common site of colonic volvulus in adults is the sigmoid colon and transverse colonic volvulus represents less than 4% of all with mortality of 35% [1-4]. Predisposing factors are mental retardation, dysmotility disorders, chronic constipation and congenital megacolon [2]. Despite the knowledge of predisposing factors with chronic constipation, a very rare incidence is the reason why this condition is only detected during an emergency open laparotomy.
A 14-year-old girl with mental retardation presented with extremely distended abdomen and vomiting. The girl is a patient of the Institute for the Care of Mentally Disabled Children and Youth Pazarić Resnik. The caregivers who accompanied the girl did not provide any information on constipation problems. A girl sent by a surgeon from Konjic General Hospital who primarily treated abdominal pain, vomiting and lack of stool.
From the history: A girl admitted to our Clinic because of problems that last 4-5 days and is accompanied by abdominal pain, vomiting and lack of stool. Vomiting once a day. Only later in the postoperative period, carefully taken heteroanamnesis and reconstruction of history we have received information that girls ha problems for chronic constipation. Subfebrile up to 37.6°C.
Physical examination revealed massively distended abdomen, tympanic, tense, diffusely painful and without bowel sounds. The abdominal wall was tender. Rectal ampulla was empty. Nasogastric tube inserted initially obtained 200 mL of dark-brown content. Bloodgas analysis revealed mixed metabolic and respiratory acidosis. Plain abdominal and chest radiography showed an enormously distended bowel (Figure 1).
 Figure 1: Plain abdominal and chest radiography
showed enormously distended bowel.
Figure 1: Plain abdominal and chest radiography
showed enormously distended bowel.During hospitalization, infusion solutions of crystalloid solutions are administered with the corrections of laboratory findings and after adequate preoperative preparation due to absolute indication, urgent surgical treatment begins. During the operation, medial laparotomy was performed, and an enormously dilated, 360 degree twisted, gangrenous altered transverse colon was found. After detection, no signs of vitality from the transverse colon are found and a resection of the transverse colon, end to end anastomosis between the spleen and hepatic flexure and protective loop ileostomy was performed (Figure 2 and 3).
>The postoperative course was satisfactory, antibiotics were administered and the peristyle was established on time. On the 20th postoperative day, a loop ileostomy was closed and a transrectal rectal biopsy was performed during the same operation On the 10th postoperative day, the patient was discharged with recommendations for continued treatment of chronic obstruction. The pathohistological analysis revealed hemorrhagic infarction and colon necrosis of the transverse colon (Figure 4 and 5)
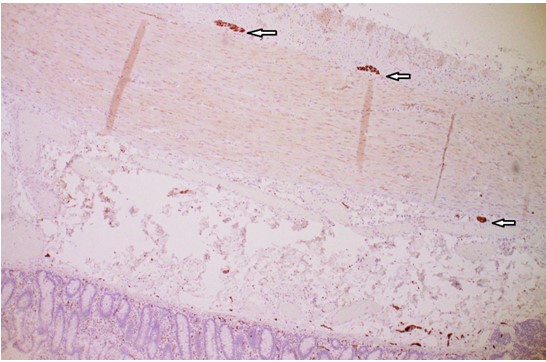 Figure 4: Positive immunostaining for calretinin in preserved ganglion cells in submucosal and myenteric plexus (arrows), HE × 10.
Figure 4: Positive immunostaining for calretinin in preserved ganglion cells in submucosal and myenteric plexus (arrows), HE × 10.Volvulus of transverse colon is a rare condition in childhood, with only a few published articles in the literature [1,2]. Chronic constipation is present as a symptom in over 50% of pediatric patients with transverse colon volvulus. Constipation can promote elongation and chronic redundancy of the transverse colon [3]. Colon becomes more mobile, thus it can easily twist upon itself. The current case also was associated with mental retardation and had a history of chronic constipation. Our patient presented with subacute transverse colon volvulus, but delayed diagnosis and treatment resulted in progressing to the acute fulminating type with bowel infarction (Figure 6).
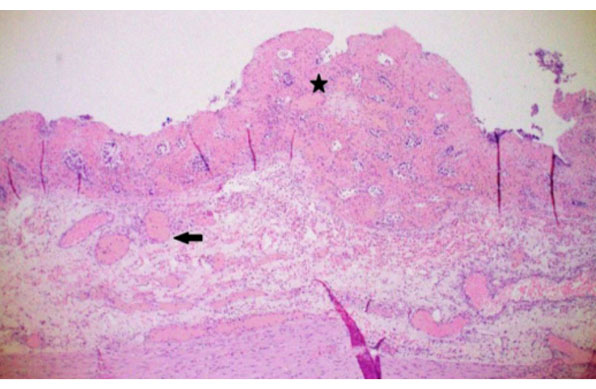 Figure 6: Colonic necrosis (star) with large dilated blood vessels (arrow) as the main histologic feature of hemorrhagic infarct, HE × 10.
Figure 6: Colonic necrosis (star) with large dilated blood vessels (arrow) as the main histologic feature of hemorrhagic infarct, HE × 10.It is a great challenge to make an accurate diagnosis of transverse colon volvulus. Diagnosis is often made with exploratory laparotomy, without knowing what it is about. In a patient with clinical deterioration, radiography may be the only diagnostic procedure that can help in setting absolute indications for urgent surgical treatment [4]. In children, colonic volvulus is a rare cause of bowel obstruction (Figure 7).
Diagnosis is challenging due to unspecific symptoms and signs, being the abdominal pain and distension the most common [4]. Risk factors associated with a transverse colonic volvulus include a narrow base of fixation, a distal colonic obstruction, and abnormalities in the intestinal muscular activity [5]. Twisting usually occurs along the mesenteric axis of the bowel, resulting in invenous obstruction and eventually arterial compromise [6]. Volvulus is favored by elongation of the colon, chronic constipation, or anatomical defects in the normal liver and colon attachments [7].
In children, a lengthy transverse colon, dysmotility disorders and chronic constipation, mental retardation and lax of fixation have all been described. 30% of children with volvulus of the transverse colon appear to have had a history of chronic constipation [8,9] which is either idiopathic or secondary to Hirschprung’s disease [10,11] mental retardation or myotonic dystrophy. Children with mental retardation will tend to have abnormal and irregular bowel function. Chronic constipation can promote elongation and chronic redundancy of the transverse colon [12].
The literature describes 2 forms of transverse colon torsion: an acute fulminating presentation in which patients typically complain of a where the patient has clinical signs of acute abdomen, a diffusely painful abdomen, vomiting, and rapid deterioration, and the subacute progressive presentation, associated with massive abdominal distension and gradual clinical symptoms [13].
Management of a transverse colonic volvulus includes endoscopic decompression with a high recurrence rate of 66% and a mortality rate of 33% [14]. Surgical options described for transverse colon volvulus include detorsion plus colopexy, resection and primary anastomosis, resection and stoma creation, or detorsion followed by elective transverse resection [15]. There is no consensus of which is the best management option for these patients. Based on our operative findings and a viable bowel with ischemic changes, we decided to perform a transverse colonic resection with a primary anastomosis and protective loop ileostomy, since the bowel was healthy and this type of surgical management has shown to decrease recurrences
Transverse colon volvulus twisted for 360 degrees in the pediatric age is an extremely rare surgically condition. The most common cause in the pediatric age is colon elongation caused by chronic obstruction, especially in patients with mental retardation. The correct diagnosis is usually made during emergency laparotomy because of the urgent clinical condition and deterioration. The most optimal scenario would be derotation and resection of a twisted colon regardless of vitality, all for the prevention of future torsion.
We declare that there is no conflict of interest regarding the publication of this paper

